Blank Official 122 Utah Form
Blank Official 122 Utah Form
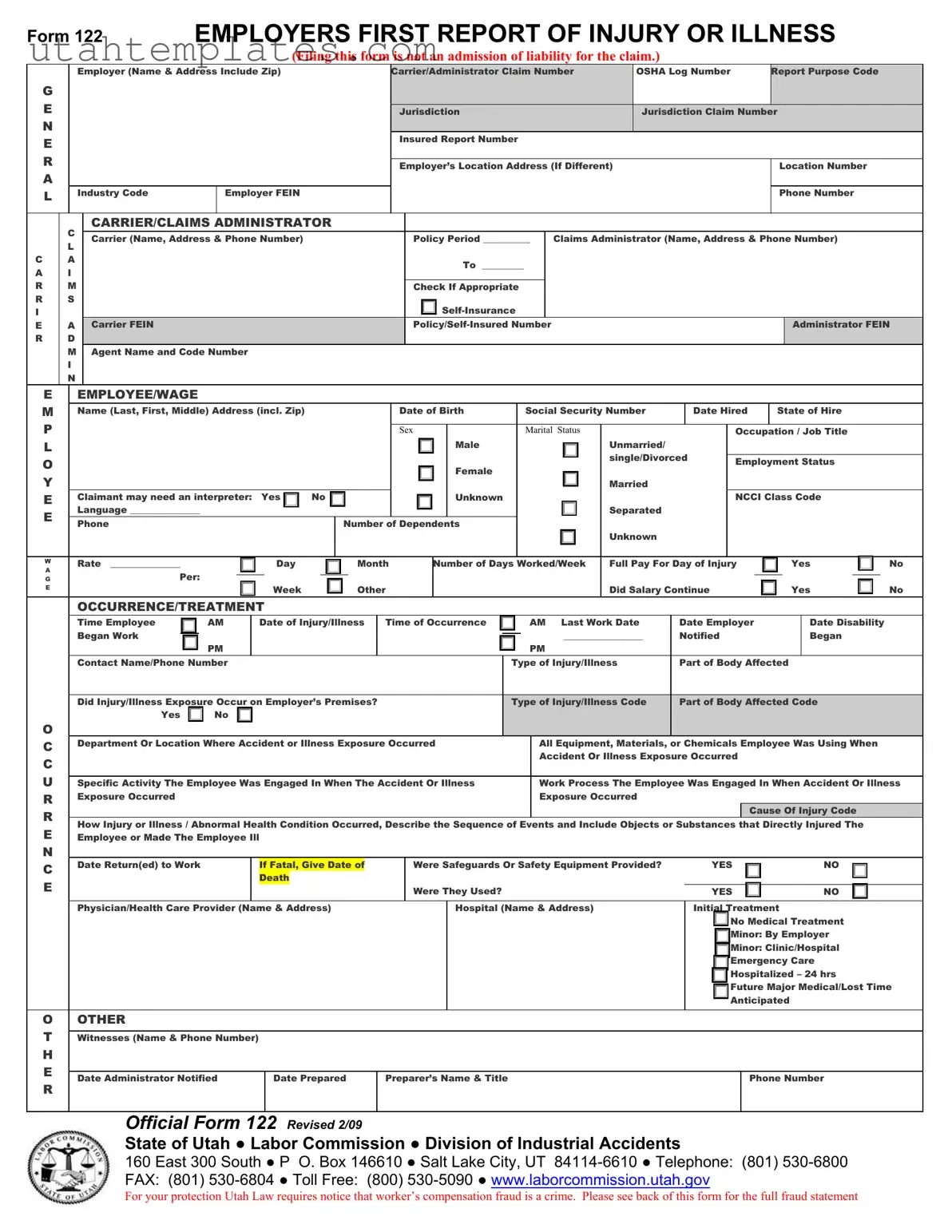
The Official 122 Utah form, also known as the Employer’s First Report of Injury or Illness, is a crucial document for both employers and employees in the state of Utah. This form must be submitted to the Labor Commission's Division of Industrial Accidents whenever an employee experiences a work-related injury or illness that requires medical treatment, results in lost time, or leads to a transfer to another job. It collects essential information such as the employer's details, the employee's information, and specifics about the injury or illness, including the time and place of occurrence, type of injury, and treatment received. Completing this form accurately and promptly is vital, as it serves not only as a record of the incident but also as a basis for any workers' compensation claims that may follow. Employers are required to file this report within seven days of the incident, and failure to do so can lead to penalties. The form also emphasizes the importance of providing thorough details, as incomplete submissions can delay the claims process. Understanding the requirements and implications of the Official 122 form can help ensure that both employers and employees navigate the workers' compensation system effectively.
Car Gift - Applicants must notify the Division of any personnel changes within ten days.
Completing the Indiana Homeschool Letter of Intent form is essential for parents looking to embark on their homeschooling journey, as it officially informs the state of Indiana of their choice. For those seeking guidance, resources are available, including a helpful link to an editable form at https://homeschoolintent.com/editable-indiana-homeschool-letter-of-intent, which can simplify the submission process and ensure all requirements are met.
How to Get Drivers License in Utah - A section allows you to indicate if you are an organ, eye, and tissue donor.
Utah State Tax Form for Employees - This form is regularly updated to reflect current tax laws and rates.
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Official 122 form, known as the Employer’s First Report of Injury or Illness, is used to report workplace injuries or illnesses to the Labor Commission in Utah. |
| Filing Timeline | Employers must submit this report within seven days of an employee's injury or notification of the injury, especially if medical treatment is involved. |
| Legal Basis | This form is governed by Sections §34A-2-407 and §34A-3-10B of the Utah Code Annotated (U.C.A.) 1997. |
| Fraud Statement | The form includes a warning that filing false claims is a crime, which may result in fines or imprisonment. |
| Confidentiality | Information submitted on this form is considered private and is only shared with parties involved in the claim. |
| Multiple Copies | Employers must provide copies of the form to the Labor Commission, the insurance carrier, the employee, and retain a copy for their records. |
| Consequences of Non-Compliance | Failure to file the report can lead to a Class C misdemeanor and potential civil penalties, as outlined in various sections of the U.C.A. |
The Official 122 Utah form is an essential document for reporting workplace injuries or illnesses. Alongside this form, several other documents are commonly used in the process of managing workers' compensation claims. Each of these forms serves a specific purpose and helps ensure that all necessary information is accurately recorded and submitted.
Using these forms in conjunction with the Official 122 Utah form helps streamline the workers' compensation process. Accurate and timely submission of these documents can significantly impact the outcome of a claim. Always ensure that all forms are completed thoroughly to avoid delays in processing.
Filling out the Official 122 Utah form can feel overwhelming, but avoiding common mistakes can make the process smoother. One of the biggest errors is failing to provide complete employer information. It’s crucial to include the correct employer name and Federal Employer Identification Number (FEIN). If this information is incorrect, it could delay the processing of the claim.
Another frequent mistake is neglecting to fill in the OSHA Log Number. This number must reflect the year of the injury and is essential for tracking purposes. Leaving this section blank can lead to complications down the road.
People often forget to provide adequate details about the employee. Missing information such as date of birth or social security number can result in the form being returned for completion. Always double-check that every field is filled out accurately.
Additionally, some individuals overlook the importance of detailing the type of injury or illness. It's not enough to simply state that an injury occurred; you must describe how it happened. Providing a clear sequence of events helps in understanding the context of the injury.
Another common oversight is not indicating whether the injury occurred on the employer’s premises. This is a critical detail that can affect the claim's outcome. Be sure to answer this question clearly.
People sometimes forget to mention whether safety equipment was provided and used. This information is vital for assessing the circumstances surrounding the injury. If safety measures were in place, it could influence the claim significantly.
When it comes to the medical treatment section, failing to specify the type of treatment received is another mistake. Whether it was minor treatment or hospitalization, accurately documenting this information is crucial for the claim process.
Providing incomplete wage information is also a common pitfall. Ensure that the wage details are accurate and complete, as this information is necessary for determining compensation benefits.
Another mistake is not keeping a copy of the completed form. It’s essential for both the employer and employee to retain a copy for their records. This can be invaluable if any questions arise later.
Lastly, some people forget to submit the form within the required timeframe. The law mandates that this report must be filed within seven days of the injury. Missing this deadline can have serious repercussions, including potential fines.
FORM 122 |
EMPLOYERS FIRST REPORT OF INJURY OR ILLNESS |
|
(Filing this form is not an admission of liability for the claim.) |
G E N E R A L
Employer (Name & Address Include Zip)
Industry Code |
Employer FEIN |
|
|
Carrier/Administrator Claim Number |
OSHA Log Number |
Report Purpose Code |
|
|
|
Jurisdiction |
Jurisdiction Claim Number |
|
|
|
|
Insured Report Number |
|
|
|
|
|
Employer’s Location Address (If Different) |
|
Location Number |
|
|
|
|
|
Phone Number |
|
|
|
C A R R I E R
C
L
A
I
M S
A D M I N
CARRIER/CLAIMS ADMINISTRATOR |
|
|
|
|
Carrier (Name, Address & Phone Number) |
Policy Period __________ |
|
Claims Administrator (Name, Address & Phone Number) |
|
|
To _________ |
|
|
|
|
|
|
|
|
|
Check If Appropriate |
|
|
|
|
|
|
|
|
Carrier FEIN |
|
Administrator FEIN |
||
|
|
|
|
|
Agent Name and Code Number
EEMPLOYEE/WAGE
M |
Name (Last, First, Middle) Address (incl. Zip) |
|
|
|
|
|
|
Date of Birth |
|
|
Social Security Number |
|
|
Date Hired |
State of Hire |
|
||||||||||||||||||||||||||||
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sex |
|
|
|
|
Marital Status |
|
|
|
|
|
Occupation / Job Title |
|
|||||||||||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
Unmarried/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
single/Divorced |
Employment Status |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
Claimant may need an interpreter: |
Yes |
No |
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
NCCI Class Code |
|
|||||||||||||||||||||||
E |
Language _______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Separated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Phone |
|
|
|
|
|
|
|
|
Number of Dependents |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
Rate _______________ |
|
|
|
|
|
Day |
|
|
|
Month |
|
Number of Days Worked/Week |
Full Pay For Day of Injury |
|
|
|
Yes |
|
|
|
No |
||||||||||||||||||||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Per: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
G |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
E |
|
|
|
|
|
|
|
|
|
|
Week |
|
|
|
Other |
|
|
|
|
|
|
|
|
Did Salary Continue |
|
|
|
|
|
|
|
Yes |
No |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
OCCURRENCE/TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Time Employee |
|
|
AM |
|
Date of Injury/Illness |
|
Time of Occurrence |
|
|
|
AM Last Work Date |
|
Date Employer |
|
|
|
Date Disability |
|
|||||||||||||||||||||||||
|
Began Work |
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_________________ |
|
|
Notified |
|
|
|
|
|
|
|
|
Began |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Contact Name/Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|
Type of Injury/Illness |
|
Part of Body Affected |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
Did Injury/Illness Exposure Occur on Employer’s Premises? |
|
|
|
|
|
Type of Injury/Illness Code |
|
|
Part of Body Affected Code |
|
|||||||||||||||||||||||||||||||||
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
Department Or Location Where Accident or Illness Exposure Occurred |
|
|
|
All Equipment, Materials, or Chemicals Employee Was Using When |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Or Illness Exposure Occurred |
|
|
|
|
|
|
|
|
|
|||||||||||
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
Specific Activity The Employee Was Engaged In When The Accident Or Illness |
|
|
|
Work Process The Employee Was Engaged In When Accident Or Illness |
||||||||||||||||||||||||||||||||||||||||
R |
Exposure Occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Exposure Occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause Of Injury Code |
|
||||||||||
How Injury or Illness / Abnormal Health Condition Occurred, Describe the Sequence of Events and Include Objects or Substances that Directly Injured The |
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||
EEmployee or Made The Employee Ill
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
Date Return(ed) to Work |
|
If Fatal, Give Date of |
|
Were Safeguards Or Safety Equipment Provided? |
YES |
NO |
|||||||||
|
|
Death |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Were They Used? |
YES |
|
|
NO |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician/Health Care Provider (Name & Address) |
|
Hospital (Name & Address) |
Initial Treatment |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
No Medical Treatment |
|||||
|
|
|
|
|
|
|
|
|
|
|
Minor: By Employer |
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Minor: Clinic/Hospital |
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Emergency Care |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Hospitalized – 24 hrs |
|||||
|
|
|
|
|
|
|
|
|
|
|
Future Major Medical/Lost Time |
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Anticipated |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OOTHER
TWitnesses (Name & Phone Number)
H |
|
|
|
|
|
E |
|
|
|
|
|
Date Administrator Notified |
Date Prepared |
Preparer’s Name & Title |
Phone Number |
||
|
|||||
R |
|
|
|
|
|
|
|
|
|
|
OFFICIAL FORM 122 REVISED 2/09
STATE OF UTAH ● LABOR COMMISSION ● DIVISION OF INDUSTRIAL ACCIDENTS
160 East 300 South ● P O. Box 146610 ● Salt Lake City, UT
FAX: (801)
For your protection Utah Law requires notice that worker’s compensation fraud is a crime. Please see back of this form for the full fraud statement
FRAUD – “Any person who knowingly presents false or fraudulent underwriting information, files or causes to be filed a false or fraudulent claim for disability compensation or medical benefits, or submits a false or fraudulent report or billing for health care fees or other professional services is guilty of a crime and may be subject to fines and confinement in state prison.”
INSTRUCTIONS TO EMPLOYER
The Employer’s First Report of Injury or Illness must be submitted to the Labor Commission, Division of Industrial Accidents, per Sections
*All information requested on this form is of vital importance. Please answer all items in detail in order to avoid additional correspondence or the return of this report for completion. Do not enter data in the shaded areas.
*The box titled “OSHA Log Number” must be filled in with the employer assigned Case Number from OSHA’s new 300 Injury Log. The Case Number needs to reflect the year of the injury – for example, your first injury in 2002 should reflect the first injury and the year 00/02 with the next injury being 00202, etc.
*Please provide WAGE information. This information is needed by the insurance company for paying the correct amount on a claim.
*The injury report on file with the Labor Commission, Division of Industrial Accidents, is private information and is only released to parties to the claim.
*Please make sure the EMPLOYER NAME is correct, as well as your FEIN # (Federal Tax ID Number). The employer’s name should be the same as reported to The Department of Workforce Services and as it appears on your WORKERS’ COMPENSATION insurance policy.
*The Labor Commission is to receive an original of this report, Worker’s Compensation Insurance Carrier gets a second copy, the employee gets a third copy, and the employer gets a fourth copy and should maintain a copy of this report.
*Failure to file this report with the Labor Commission or failure to provide the employee with a copy of the report, is a Class C misdemeanor and can also result in a citation and a civil penalty for each violation as per
*If you dispute the validity of this claim you need to contact your insurance carrier, but you must still file the “Employer’s First Report of Injury or Illness” form with the Labor Commission.
*Reminder: Inform your injured employee of his/her rights and obligations (as outlined on the back of the employee’s copy) of Utah’s Workers’ Compensation Act.
For Additional Information please contact:
State of Utah – Labor Commission Division of Industrial Accidents 160 East 300 South, 3rd Floor
P O Box 146610
Salt Lake City, Utah
FRAUD – “Any person who knowingly presents false or fraudulent underwriting information, files or causes to be filed a false or fraudulent claim for disability compensation or medical benefits, or submits a false or fraudulent report or billing for health care fees or other professional services is guilty of a crime and may be subject to fines and confinement in state prison.”
EMPLOYEE INFORMATION
•INJURY/ILLNESS REPORT: A report of your injury/occupational illness must be made with your employer. If a report of injury is not filed with your employer or the Labor Commission, Division of Industrial Accidents, within 180 days of the date of your injury/illness, you may lose the right to ever file a claim for workers’ compensation benefits for that injury or illness.
•EMPLOYER’S PHYSICIAN: If your employer has a company physician or designated clinic for industrial accidents, you MUST see the company physician first, or you may not be eligible for workers’ compensation benefits. After you have been seen by your employer’s physician, you have the right to choose one treating physician.
•MEDICAL COOPERATION: You must cooperate with your employer or the insurance carrier in following prescribed medical treatment in order to return to work as quickly as possible.
•TRAVEL REIMBURSEMENT: You may be eligible for travel reimbursement to and from approved medical care. You will need to keep records. Contact your insurance carrier regarding travel expenses.
•REEMPLOYMENT ASSISTANCE: You may be eligible for reemployment assistance if you are unable to return to work due to an industrial injury. Contact your insurance carrier or the Labor Commission, Division of Industrial Accidents, for further information.
•MEDICAL EXPENSES: You are entitled to have all reasonable medical expenses paid that are a result of the injury or illness.
•COMPENSATION BENEFITS: You are entitled to
□If you have sustained a permanent impairment due to the industrial injury or disease, you are entitled to compensation based on the impairment rating as determined by a physician.
□If you are permanently totally disabled from working due to the industrial injury, you may need to apply at the Labor Commission, Division of Industrial Accidents, for a hearing to determine if benefits are due.
•ADDITIONAL ASSISTANCE: If you are unable to work due to an industrial injury and meet the program’s requirements, you may be eligible for other assistance. Agencies you may wish to contact:
□Department of Workforce Services for food stamps, cash assistance, medical assistance, or employment assistance.
□Social Security for total disability benefits.
•UNEMPLOYMENT BENEFITS: If you are able to work, but have been terminated from your job, you need to apply at the nearest Department of Workforce Services employment office within 90 calendar days after you are released from
Contact your insurance carrier if problems occur during your injury regarding payment of medical bills or compensation benefits. If you need to know who your employer’s insurance carrier is, you may ask your employer or contact the Labor Commission, Division of Industrial Accidents.
THIS IS AN IMPORTANT DOCUMENT TO MAINTAIN FOR YOUR RECORDS
OSHA Form 300: This form is used to log work-related injuries and illnesses. Like the Official 122 form, it requires detailed information about the incident, including the nature of the injury and the affected body part. Both forms aim to ensure proper reporting and tracking of workplace incidents.
Workers' Compensation Claim Form: This document initiates a claim for workers' compensation benefits. Similar to the Official 122 form, it gathers essential information about the injury, including the date and circumstances. Both forms are crucial for securing benefits for injured employees.
First Report of Injury (State-Specific): Many states have their own versions of a first report of injury form. These documents share the same purpose as the Official 122 form, which is to notify relevant authorities about an employee's injury or illness promptly.
Incident Report Form: This form is typically used by employers to document workplace incidents. Like the Official 122 form, it captures details about the event, including witnesses and circumstances, to help prevent future occurrences.
Medical Treatment Authorization Form: This document is used to authorize medical treatment for an injured employee. It is similar to the Official 122 form in that it requires information about the injury and the employee, ensuring that appropriate care is provided.
Return to Work Form: This form is used to confirm an employee's ability to return to work after an injury. It parallels the Official 122 form in that both require information about the injury and the employee's status, facilitating a smooth transition back to work.
Employer's Report of Injury Form: This document is often required by insurance carriers to report workplace injuries. It is similar to the Official 122 form, as both serve to inform relevant parties about the specifics of an incident.
Claim for Compensation Form: This form is used to request compensation for lost wages due to a work-related injury. Like the Official 122 form, it gathers important details about the injury and its impact on the employee's ability to work.
Accident Investigation Report: This report documents the findings of an investigation into a workplace accident. It is similar to the Official 122 form in that both seek to understand the causes of incidents and improve workplace safety.
Articles of Incorporation: The Ohio Articles of Incorporation form is essential for establishing a corporation in Ohio, as it provides necessary details about the corporation such as its name, purpose, and structure. For more information, check out Ohio PDF Forms.
Safety Incident Report: This form is used to document any safety incidents in the workplace. Like the Official 122 form, it collects information about the incident to help identify trends and improve safety protocols.
Filling out the Official 122 Utah form is a critical step for employers and employees in the event of a workplace injury or illness. Here are ten key takeaways to ensure proper completion and understanding of this form:
Understanding these key points can help ensure compliance with Utah's regulations and protect the rights of both employers and employees. Prompt and accurate reporting is not just a legal obligation; it also plays a vital role in the recovery process for injured workers.